4 Weeks 8 Weeks
STUDENT INFORMATION
PARENT INFORMATION
17. RELATIEVS AND FRIENDS PHONE # TO CONTACT IN A CASE OF AN EMERGENCY:
AGREEMENT
I, residing at agree to register my son/daughter with BECEC Inc., d/b/a ALPHA SUMMER CAMP.
I undertake to pay $ and understand that this amount covers expenses for staying of my son/daughter for: 4 Weeks 8 Weeks
These balances of all fees are payable prior to the camper’s first day of the scheduled attendance.
BECEC Inc., d/b/a ALPHA SUMMER CAMP RESERVED THE RIGHT TO REFUSE ADMISSION TO ANY CAMPER WHOSE PAYMENT HAS NOT BEEN RECEIVED.
I also understand that there is no deduction for any absence in case of illness, vacation or other reasons. Full payment is due despite of government or religious holidays included in BECEC Inc., d/b/a ALPHA SUMMER CAMP Schedule.
No adjustments, allowance or refund of the deposit or balance shall be made except in strict conformity with the rules:
- If a parent of a camper notifies in writing BECEC Inc., d/b/a ALPHA SUMMER CAMP, prior June 15, those child/children will be unable to attend for any reasons whatsoever, a full refund will be made of all fees previously paid.
- If a parent of a camper notifies BECEC Inc., d/b/a ALPHA SUMMER CAMP, that child/children are unable to attend because of injury or illness, properly documented, all money received on behalf of the applicant will be refunded.
I understand that for the safety, welfare and proper maintenance of all campers, the BECEC Inc., d/b/a ALPHA SUMMER CAMP., reserves the right, in its sole discretion, to suspend or expel camper whose conduct or influence is damaging and/or potential dangerous to the safety of campers, camp staff or camp property. The BECEC Inc., d/b/a ALPHA SUMMER CAMP reserves the right to determine the severity of the disciplinary issues and threats to the safety of its campers, in its sole and absolute discretion. Some egregious examples of misconduct include but are not limited to: physical violence toward campers and camp staff, damage or defacing of camp property, theft, inappropriate behavior, carrying/use of weapons or materials which may be used as weapons. On the part of the parent, an obvious misrepresentation regarding the medical or mental history of a camper will result in action to be taken against the camper that may include dismissal from the camp. The previously stated examples of misconduct are just examples and BECEC Inc., d/b/a ALPHA SUMMER CAMP may deem other conduct or misrepresentation as damaging or dangerous, in its sole and absolute discretion. All of the abovementioned disruptions to the safety standards of the BECEC Inc., d/b/a ALPHA SUMMER CAMP may lead to the student’s dismissal from the camp. The BECEC Inc., d/b/a ALPHA SUMMER CAMP administrative staff reserves the right to make judgments upon disciplinary action, in its sole and absolute discretion, to be taken against a student (including suspensions or dismissals). In the event of school suspensions or dismissals, no refunds or adjustments will be made to the school tuition fees. In cases of damage done to the school property, the camp director or administrative staff reserves the right to assess the level of damage caused to the camp property. All costs for repairs will be charged to camper account. The BECEC Inc., d/b/a ALPHA SUMMER CAMP shall have further right to charge and receive collection of attorney’s fees on any unpaid balances plus interest, expenses and court costs, if any, in the event that the school initiates proceedings for the collection on any unpaid balances due.
Due to the seasonal nature of the business, no refund or credit will made for any portion of the camping period not completed, including late admission, early departure (leaving), and dismissal for cause, disability or withdrawal for any reason. Tuition and fees already paid and or due is agreed to be the fair and reasonable sum as and for liquidated damages. All claims for refund or credit are expressly waived and released by the parents and or guardian of the child.
BECEC Inc., d/b/a ALPHA SUMMER CAMP shall not be responsible for clothing or personal possessions lost or damaged by fire, theft, malicious mischief or personal negligence.
In cases of extreme emergency, I give permission to the physician or hospital selected by the school officials to hospitalize, secure proper treatment for, order injections, anesthesia, X-rays or surgery to my child. I understand that the cost of medical services will be entirely my responsibility. I understand that the BECEC Inc., d/b/a ALPHA SUMMER CAMP will make every effort to contact me or another designated emergency contact person before or immediately after such emergency treatment is rendered.
Permission hereby granted to BECEC Inc., d/b/a ALPHA SUMMER CAMP, Inc. to use any photograph, film or video, of the above camper in any public release, publicity, advertisements of brochure, television program or promotional video.
If a Parent decides to withdraw his or her child, the directors require 24-hour notice. The child may be picked up from campsite only. Parent/guardian further agrees to waive the right to press legal charges against BECEC Inc., d/b/a ALPHA SUMMER CAMP. its officers, directors, and employers, in those instances where any of the above have not clearly demonstrated negligence leading to injury of the above named child.
The camp assumes no responsibility for the acts done by campers when in violation of camp rules, local, State or Federal laws. The camp is not responsible for losses of personal property or acts done by campers or other persons while off camp’s premises. Parent/guardian will be responsible for any damages incurred by camper on or off camp premises.
BECEC Inc., d/b/a ALPHA SUMMER CAMP, is required to be licensed by the New York City Department of Health.
BECEC Inc., d/b/a ALPHA SUMMER CAMP, accepts no responsibility or liability for any: accident, illness or mishap, which is not the fault of BIG APPLE SUMMER CAMP.
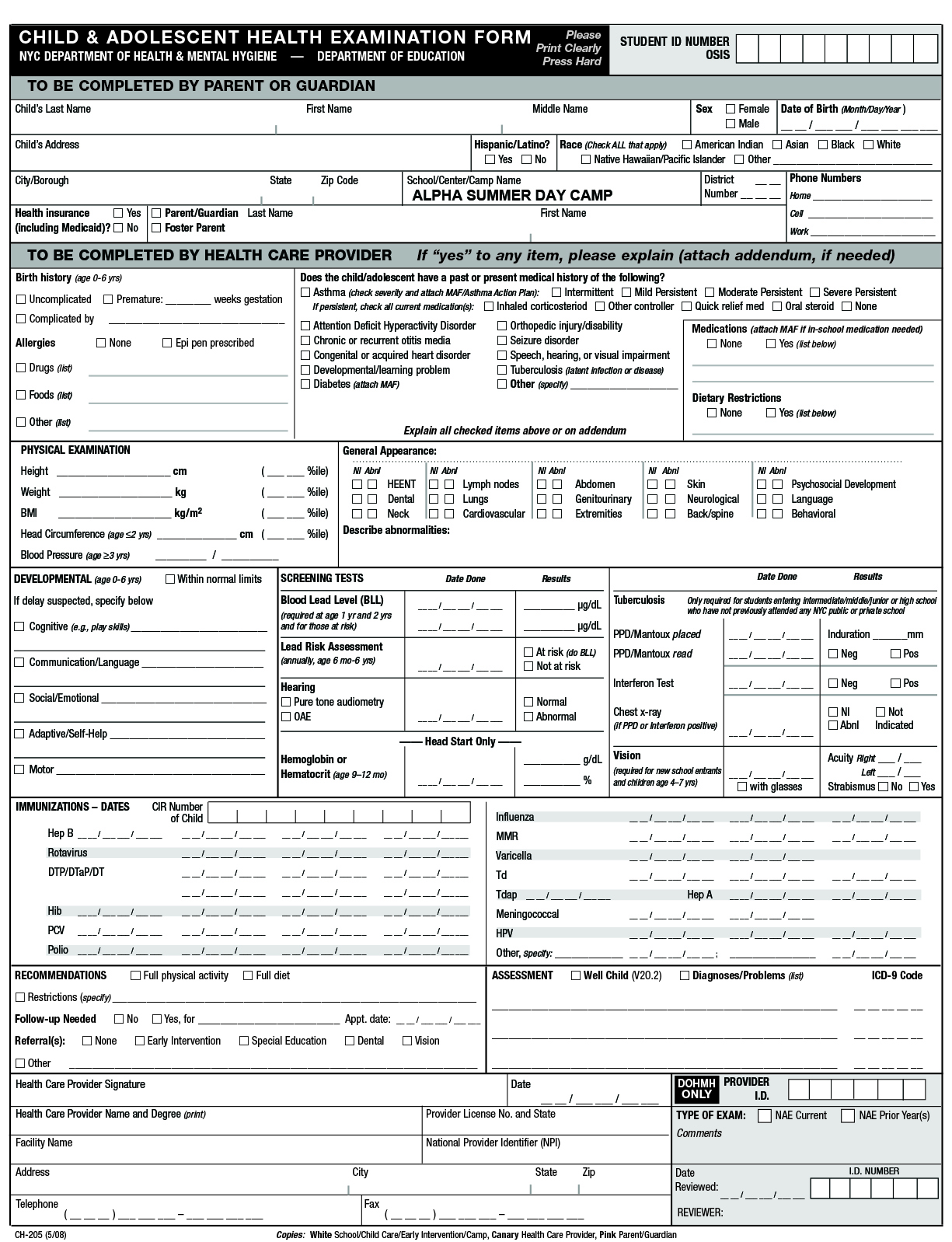
I hereby confirm that the above named child/children is in good physical condition and has been examined by a physician within the past 6 (six) months and is in relatively good health and able to participate in a full BECEC Inc., d/b/a ALPHA SUMMER CAMP programs.
I have read and understood the Agreement of the Enrollment terms, which have been presented in the Agreement. I agree to all terms contained in the Agreement. In agreeing to the terms presented in the Agreement, I acknowledge that I am also acting on the behalf of the other parent/legal guardian (if that person is not present at the signing of the Agreement) with the authority to enroll my child in to the BECEC Inc., d/b/a ALPHA SUMMER CAMP and agree to execute this agreement on his or her behalf. I recognize that the BECEC Inc., d/b/a ALPHA SUMMER CAMP relies upon the representation herein made in accepting my child to the BECEC Inc., d/b/a ALPHA SUMMER CAMP
Parent’s Signature Ok
Date
EMERGENCY MEDICAL RELEASE AGREEMENT
As the parent or legal guardian of:
I, , give my permission for my child to receive whatever emergency medical care that may be deemed needed by BECEC Inc., d/b/a ALPHA SUMMER CAMP, personnel for the treatment of any injury that may be incurred while in the Camp’s activities or swimming on premises or elsewhere.
I understand BECEC Inc., d/b/a ALPHA SUMMER CAMP, will make effort to contact myself or my emergency contact before or immediately after such emergency treatment is rendered.
LIMITED WAIVER OF LIABILITY
The BECEC Inc., d/b/a ALPHA SUMMER CAMP, provides serious education, recreation and sports programs including swimming. Our staff is trained in safety techniques to provide the maximum of protection for your child while in our care. Even with all of these safeguards injuries can occur.
As a parent or legal guardian of the above named camper, I fully understand the risks involved in my child’s participation in the all Camp Activities or swimming. To the best of my knowledge my child has no medical conditions, which would conflict with his/her participating in the full summer programs. I further agree to waive the right to press any legal proceedings against BECEC Inc., d/b/a ALPHA SUMMER CAMP, its officers and staff, in those instances where any of the above has not clearly demonstrated negligence leading to injury of the above named student.
Signature Ok
BUS AGREEMENT
As the parent or legal guardian of:
I request to provide bus services for my son/daughter. I understand that no door- to -door services is available. I understand that bus will pick-up/drop-off my child at an assigned bus stop and the child will be released from the bus only to a parent or to a person authorized to pick up the child. In case there is nobody at the bus stop to pick up the child he/she will be taken to a designated waiting room located at the bus parking lot. In such an event there will be additional charge of $30 for every 30 minutes the child spends in the waiting room (NO EXEPTIONS). Camp will not provide a professional staff for waiting room services.
In Accordance with 22:16 of the School Law the School Administration has the authority to suspend the transportation privileges of child/children who are disorderly and insubordinate. When camp suspends a student’s transportation privileges, the parents or guardian of the child involved become responsible for seeing that the child gets to and from camp.
Signature Ok
TRANSPORTATION REQUEST FORM
The undersigned parent(s) or legal guardian(s) Of hereby authorize BECEC Inc., d/b/a ALPHA SUMMER CAMP, (“Organizers”), to facilitate the procurement of bus transportation for my son/daughter. In their role as facilitators, I/we hereby authorize Organizers to enter into a Pupil Transportation Services Agreement with Academy Transportation Inc. on my/our behalf.
I/we hereby indemnify and hold Organizers harmless for the acts or omissions of Academy Transportation Inc. in the performance of the bus transportation services for Camper(s).
PARENT/GUARDIAN INFORMATION:
Parent’s Name:
Address:
CityState Zip Code
Work Phone #
Cell Phone#
STUDENT INFORMATION:
Child’s Name: Grade
SCHOOL BUS TRANSPORTATION LIABILITY WAIVER
As parent/guardian of the above named child/children, I hereby release the BECEC Inc., d/b/a ALPHA SUMMER CAMP, its agents, employees and trustees from all liability arising out of his/her transportation on the school bus to or from the BECEC Inc., d/b/a ALPHA SUMMER CAMP and throughout all the extra curriculum activities including daily trips.
As parent and/or legal guardian, I remain legally responsible for any personal actions taken by the above named Camper(s). I agree on behalf of myself, my child named herein, or our heirs, successors and assigns, to hold harmless and defend BECEC Inc., d/b/a ALPHA SUMMER CAMP, its officers, event, from any and all actions, claims, demands, damages, costs, expenses and all consequential damage arising from or in connection therewith, and I agree to compensate the camp, its officers, directors and agents, chaperones, or representatives associated with the event for reasonable attorney’s fees and expenses arising therewith
I understand that it is my full responsibility as parent/guardian to:
- Place him/her on the bus in the morning, and to meet him/her in the evening at the bus stop.
- Be on time for the evening pickup
- Instruct my child/children as to his/her pickup and drop off point
- Review with my child/children the School Bus Rules provided by the camp.
Ok
STUDENT RELEASE FORM
BECEC Inc., d/b/a ALPHA SUMMER CAMP., recommends all participants obtain a physical examination from their physician prior to participating in any or all programs provided by BECEC Inc., d/b/a ALPHA SUMMER CAMP., or its affiliates.
1. The sports programs at BECEC Inc., d/b/a ALPHA SUMMER CAMP., requires the participant to perform a great deal of physical exertion, including sprints, hand-eye coordination activities, and agility drills. This form of exercise directly affects heart rate, body temperature and respiration, and requires the participant to be in good physical condition. It is up to the participant, or parent/guardian, to ensure that he/she is physically capable and in good mental condition, so as to permit safe participation in the program. BECEC Inc., d/b/a ALPHA SUMMER CAMP., shall have no responsibility, nor liability to confirm the medical condition of a participant. The undersigned recognizes the possible dangers connected with physical activity and competition and it is expressly agreed that participation in the program shall be undertaken at the participant’s own risk. In consideration of the undersigned’s participation in the program, the undersigned hereby certifies and represents that he/she is in good medical condition and is physically capable of safely participating in the program, and utilizing all exercise equipment, athletic equipment, and training required in the program.
2. The undersigned hereby releases BECEC Inc., d/b/a ALPHA SUMMER CAMP., it’s directors, employees, agents, representatives, coaches, and volunteers, as well as the owners of any facilities in which the program is conducted, on behalf of himself/herself and any one claiming by, through or under the undersigned, from any and all claims of damage, injury, or death, of any kind, arising out of the undersigned’s participation in the program. In addition, the undersigned acknowledges and agrees to indemnify and hold BECEC Inc., d/b/a ALPHA SUMMER CAMP., harmless from any claims of damage, injury or death arising out of the participation of the undersigned in the program, including injuries caused in whole or in part by the undersigned, or another participant.
3. Moreover, by this release, the undersigned also intends to fully, completely and forever release, discharge, and absolve BECEC Inc., d/b/a ALPHA SUMMER CAMP., all of its directors, employees, agents, representatives, coaches, and volunteers, from any active or passive negligence whatsoever on the part of BECEC Inc., d/b/a ALPHA SUMMER CAMP., its directors, employees, agents, representatives, coaches, and volunteers. The undersigned further agrees and promises not to sue or exercise any legal rights to seek damages or relief of any nature from BECEC Inc., d/b/a ALPHA SUMMER CAMP., its directors, employees, agents, representatives, coaches, and volunteers. The undersigned certifies that he/she has read this release and all of the statements contained herein, and further represents that he/she understood its contents and has voluntarily executed this release. The undersigned understands that he/she is giving up valuable rights and is signing this release voluntarily. The undersigned further agrees that no oral representations, statements, or inducements of any kind apart from this written release have been made with regard to the subject matter of this release.
4. The undersigned hereby warrants that he/she is over the age of eighteen, is competent to contract in his/her name, and that the undersigned has the authority to grant this consent and release.
Signature: Ok
Relationship to minor:
Part 2. Foster Child
Foster children eligible for free and reduced-price meals regardless of household income. If a foster child lives with you, please contact [name of Sponsor] at [phone number]. Complete Part 3 if you are applying for other children in your household and you did not enter a SNAP (Food Stamp), TANF or FDPIR case number in Part 1.
|
| Part 3. Total Household Gross Income—You must tell us how much and how often |
A. Name
(List everyone in household,
including children) |
B. Gross income and how often it was received
Example: $100/monthly $100/twice a month $100/every other week $100/weekly |
C. Check if NO income. |
| 1. Earnings from workbefore deductions |
2. Welfare, child support, alimony |
3. Social Security, pensions, retirement, |
4. All Other Income |
|
1.
|
$/
|
$/
|
$/
|
$/
|
Ok
|
|
2.
|
$/
|
$/
|
$/
|
$/
|
Ok
|
|
3.
|
$/
|
$/
|
$/
|
$/
|
Ok
|
|
4.
|
$/
|
$/
|
$/
|
$/
|
Ok
|
|
5.
|
$/
|
$/
|
$/
|
$/
|
Ok
|
|
6.
|
$/
|
$/
|
$/
|
$/
|
Ok
|
|
7.
|
$/
|
$/
|
$/
|
$/
|
Ok
|
|
8.
|
$/
|
$/
|
$/
|
$/
|
Ok
|
|
9.
|
$/
|
$/
|
$/
|
$/
|
Ok
|
|
10.
|
$/
|
$/
|
$/
|
$/
|
Ok
|
|
11.
|
$/
|
$/
|
$/
|
$/
|
Ok
|
|
12.
|
$/
|
$/
|
$/
|
$/
|
Ok
|
Part 4. Signature and Social Security Number (Adult must sign)
An adult household member must sign this form. If Part 3 is completed, the adult signing the form must also list the last four digits of his or her Social Security Number or mark the “I do not have a Social Security Number” box. (See Privacy Act Statement on the back of this page.) I certify that all information on this form is true and that all income is reported. I understand that this information is being given for the receipt of Federal funds. I understand that SFSP officials may verify the information. I understand that if I purposely give false information, the participant receiving meals may lose the meal benefits, and I may be prosecuted.
Sign here: X Print name: Date:
Address: Phone Number:
Last four digits of Social Security Number: Ok I do not have a Social Security Number
|
|
Part 5. Participant’s ethnic and racial identities (optional)
|
|
Mark one ethnic identity:
|
Mark one or more racial identities:
|
Ok Hispanic or Latino
Ok Not Hispanic or Latino
|
Ok Asian
Ok White
Ok Black or African American
|
Ok American Indian or Alaska Native
Ok Native Hawaiian or Other Pacific Islander
|
|
Don’t fill out this part. This is for official use only.
|

|
INCOME ELIGIBILITY FORM
SUMMER FOOD SERVICE PROGRAM
(For Use by Camps and Closed Enrolled Sites)
Please complete the following form using the instructions below. Sign the form and return it to: [Name of Sponsor]
If you need help, call [phone number of Sponsor]
Follow these instructions, if your household gets SNAP (Food Stamps) TANF or FDPIR:
Part 1: List participant’s name and a SNAP (Food Stamp), TANF or FDPIR case number.
Part 2: Skip this part.
Part 3: Skip this part.
Part 4: Sign the form. A Social Security Number is NOT required.
Part 5: Answer this question if you choose to
If your household includes a FOSTER CHILD, use one application for the whole household and follow these instructions:
Part 1: Enter the child’s name.
Part 2: Please contact us at [phone number of Sponsor]
Part 3: Complete this part if you are applying for other children in the household and you did not enter a SNAP (Food Stamp), TANF or FDPIR case number in Part 1.
Part 4: Sign the form. If Part 3 was completed, provide the last four digits of the signing adult’s Social Security Number.
Part 5: Answer this question if you choose to.
ALL OTHER HOUSEHOLDS, including WIC households, follow these instructions:
Part 1: List each participant’s name.
Part 2: Skip this part.
Part 3: Follow these instructions to report total household income from last month.
Column A–Name: List the first and last name of each person living in your household, related or not (such as grandparents, other relatives, or friends who live with you). You must include yourself and all children living with you. Attach another sheet of paper if you need to.
Column B–Gross income last month and how often it was received. Next to each person’s name, list each type of income received last month, and how often it was received. In Box 1, list the gross income each person earned from work. This is not the same as take-home pay. Gross income is the amount earned before taxes and other deductions. The amount should be listed on your pay stub, or your boss can tell you. Next to the amount, write how often the person got it (weekly, every other week, twice a month, or monthly).
In box 2, list the amount each person got last month from welfare, child support, alimony.
In box 3, list Social Security, pensions, and retirement.
In box 4, list ALL OTHER INCOME SOURCES including Worker’s Compensation, unemployment, strike benefits, Supplemental Security Income (SSI), Veteran’s benefits (VA benefits), disability benefits, regular contributions from people who do not live in your household. Report net income for self-owned business, farm, or rental income. Next to the amount, write how often the person got it. If you are in the Military Housing Privatization Initiative do not include this housing allowance.
Column C–Check if no income: If the person does not have any income, check the box.
Part 4: An adult household member must sign the form and include the last four digits of his or her Social Security Number, or mark the box if he or she doesn’t have one.
Part 5: Answer this question if you choose to.
Privacy Act Statement: The Richard B. Russell National School Lunch Act requires the information on this application. You do not have to give the information, but if you do not, we cannot approve your child for free or reduced price meals. You must include the social security number of the adult household member who signs the application. The social security number is not required when you apply on behalf of a foster child or you list a SNAP, Temporary Assistance for Needy Families (TANF) Program or Food Distribution Program on Indian Reservations (FDPIR) case number for your child or other (FDPIR) identifier or when you indicate that the adult household member signing the application does not have a social security number. We will use your information to determine if your child is eligible for free or reduced price meals, and for administration and enforcement of the Program.
Non-discrimination Statement: In accordance with Federal civil rights law and U.S. Department of Agriculture (USDA) civil rights regulations and policies, the USDA, its Agencies, offices, and employees, and institutions participating in or administering USDA programs are prohibited from discriminating based on race, color, national origin, sex, disability, age, or reprisal or retaliation for prior civil rights activity in any program or activity conducted or funded by USDA.
Persons with disabilities who require alternative means of communication for program information (e.g. Braille, large print, audiotape, American Sign Language, etc.), should contact the Agency (State or local) where they applied for benefits. Individuals who are deaf, hard of hearing or have speech disabilities may contact USDA through the Federal Relay Service at (800) 877-8339. Additionally, program information may be made available in languages other than English.
To file a program complaint of discrimination, complete the USDA Program Discrimination Complaint Form, (AD-3027) found online at: http://www.ascr.usda.gov/complaint_filing_cust.html, and at any USDA office, or write a letter addressed to USDA and provide in the letter all of the information requested in the form. To request a copy of the complaint form, call (866) 632-9992. Submit your completed form or letter to USDA by:
(1) mail: U.S. Department of Agriculture
Office of the Assistant Secretary for Civil Rights
1400 Independence Avenue, SW
Washington, D.C. 20250-9410;
(2) fax: (202) 690-7442; or
(3) email: program.intake@usda.gov.
This institution is an equal opportunity provider